Healthcare Institutional System
A Healthcare Institutional System is a social institutional system that provides healthcare services (through healthcare organizations and healthcare resources to meet population health needs).
- AKA: Health System, Healthcare System, Health Care System.
- Context:
- It can organize Healthcare Resources through service delivery structures.
- It can coordinate Healthcare Providers through organizational frameworks.
- It can deliver Health Services through care delivery processes.
- It can manage Healthcare Access through service provision models.
- It can maintain Healthcare Quality through standard enforcement.
- ...
- It can often involve Primary Healthcare through basic care provision.
- It can often include Public Health Measures through population health management.
- It can often require Healthcare Planning through resource allocation.
- It can often integrate Healthcare Stakeholders through coordination mechanisms.
- It can often adapt to Population Needs through service evolution.
- ...
- It can range from being a Public Healthcare System to being a Private Healthcare System, depending on its funding model.
- It can range from being a Centralized Healthcare System to being a Decentralized Healthcare System, depending on its organizational structure.
- It can range from being a Basic Healthcare System to being an Advanced Healthcare System, depending on its capability level.
- It can range from being a Local Healthcare System to being a National Healthcare System, depending on its geographic scope.
- It can range from being a Traditional Healthcare System to being a Modern Healthcare System, depending on its technological adoption.
- It can range from being a Resource-Constrained Healthcare System to being a Resource-Rich Healthcare System, depending on its resource availability.
- ...
- It can interact with Government Policy through regulatory compliance.
- It can support Public Health through population interventions.
- It can enable Clinical Care through service infrastructure.
- It can facilitate Health Research through evidence generation.
- ...
- Examples:
- National Healthcare Systems, such as:
- Universal Healthcare Systems, such as:
- Canadian Healthcare System providing universal access.
- UK National Health Service delivering public healthcare.
- Mixed Healthcare Systems, such as:
- US Healthcare System combining public and private provision.
- German Healthcare System integrating multiple payers.
- Universal Healthcare Systems, such as:
- Healthcare Delivery Models, such as:
- Integrated Care Systems, such as:
- Kaiser Permanente Model coordinating comprehensive care.
- Veterans Health Administration providing veteran care.
- Community Health Systems, such as:
- Rural Health Network serving remote populations.
- Urban Health System addressing city health needs.
- Integrated Care Systems, such as:
- Specialized Healthcare Systems, such as:
- Mental Health Systems, such as:
- Psychiatric Care Network providing mental health services.
- Behavioral Health System supporting psychological care.
- Emergency Care Systems, such as:
- Trauma Care Network handling critical care.
- Emergency Response System managing urgent care.
- Preventive Care Systems, such as:
- Public Health Network delivering preventive services.
- Wellness System promoting health maintenance.
- Mental Health Systems, such as:
- ...
- National Healthcare Systems, such as:
- Counter-Examples:
- Monetary System, which manages financial resources rather than healthcare.
- Healthcare Software System, which provides technical support rather than direct care.
- Surveillance System, which monitors population rather than delivers healthcare.
- Legal Institutional System, which administers justice rather than healthcare services.
- Educational Institutional System, which provides learning rather than medical care.
- See: Public Health, Clinical Trial, Governmental Organization, World Health Organization (WHO), Healthcare Policy, Medical System, Health Insurance System.
References
2020
- (Wikipedia, 2020) ⇒ https://en.wikipedia.org/wiki/Health_system Retrieved:2020-8-26.
- A health system, also sometimes referred to as health care system or as healthcare system, is the organization of people, institutions, and resources that deliver health care services to meet the health needs of target populations.
There is a wide variety of health systems around the world, with as many histories and organizational structures as there are nations. Implicitly, nations must design and develop health systems in accordance with their needs and resources, although common elements in virtually all health systems are primary healthcare and public health measures. In some countries, health system planning is distributed among market participants. In others, there is a concerted effort among governments, trade unions, charities, religious organizations, or other co-ordinated bodies to deliver planned health care services targeted to the populations they serve. However, health care planning has been described as often evolutionary rather than revolutionary.[1] [2] As with other social institutional structures, health systems are likely to reflect the history, culture and economics of the states in which they evolve. These peculiarities bedevil and complicate international comparisons and preclude any universal standard of performance.
- A health system, also sometimes referred to as health care system or as healthcare system, is the organization of people, institutions, and resources that deliver health care services to meet the health needs of target populations.
- ↑ "Health care system". Liverpool-ha.org.uk. Retrieved 6 August 2011.
- ↑ New Yorker magazine article: "Getting there from here." 26 January 2009
2017
- (Ortiz-Ospina & Roser, 2017) ⇒ Esteban Ortiz-Ospina, and Max Roser (2017). "Financing Healthcare". Published online at OurWorldInData.org.
- QUOTE: Health is a fundamental driver of our overall quality of life. In this entry we focus on healthcare – one of the most important inputs to produce health. There are many other factors affecting health, and you can read more about some of them in our entries about health.
Publicly funded healthcare is a legacy of the Age of Enlightenment.1 The first examples of legislation on health insurance date back to the late 19th century.2 Data from these early systems shows that healthcare expenditure only began rising several years after the expansion of insurance coverage, with the discovery of powerful new treatments.3
The impact that scientific developments had on healthcare expenditure is epitomized in the U.S. experience: in recent decades, as treatment possibilities expanded rapidly, expenditure on healthcare increased (private and public, both per capita and as a share of gross domestic product); and this occurred without major changes in insurance coverage. This had two important consequences: (i) the U.S. currently spends more government money per person on healthcare than many countries that fund universal programs, and (ii) spending is so concentrated that the top 1% of spenders account for more than 20% of total healthcare expenditure.4
Global expenditure on healthcare as a share of world income has been increasing, steadily but slowly over the course of the last couple of decades. In the background, however, there has been substantial cross-country heterogeneity, both in levels and trends. Regionally, high-income countries spend – and have been spending – a much larger share of their income on healthcare than low-income countries (about twice as much). Moreover, in contrast to high-income countries, in low and middle-income countries the public share of healthcare funding is much lower – although it has been catching up – and the role of out-of-pocket expenditures is much higher (above 50% of total expenditure in many countries).5
Healthcare financing in developing countries in the 21st century has been largely shaped by the flow of resources channeled through development assistance. These flows – which saw a steep increase after the introduction of the Millennium Development Goals – account for around 0.7% of the resources spent by high-income countries on healthcare. Although this may seem small in proportion to the national commitments of rich countries, for low-income countries at the receiving end of the transfers, these resources are substantial; in Sub-Saharan Africa they finance more than 25% of total expenditure on healthcare.6 This implies that development assistance for health, if suitably targeted and managed, has the potential of drastically reducing inequality in health outcomes: the robust empirically observed relationship between health outcomes and healthcare spending is indicative of large returns to healthcare investments, particularly at low levels of baseline expenditure.7
- QUOTE: Health is a fundamental driver of our overall quality of life. In this entry we focus on healthcare – one of the most important inputs to produce health. There are many other factors affecting health, and you can read more about some of them in our entries about health.
2016
- (Ortiz-Ospina & Roser, 2016) ⇒ http://ourworldindata.org/financing-healthcare/#cross-country-evidence-suggests-substantial-health-returns-to-healthcare-investment
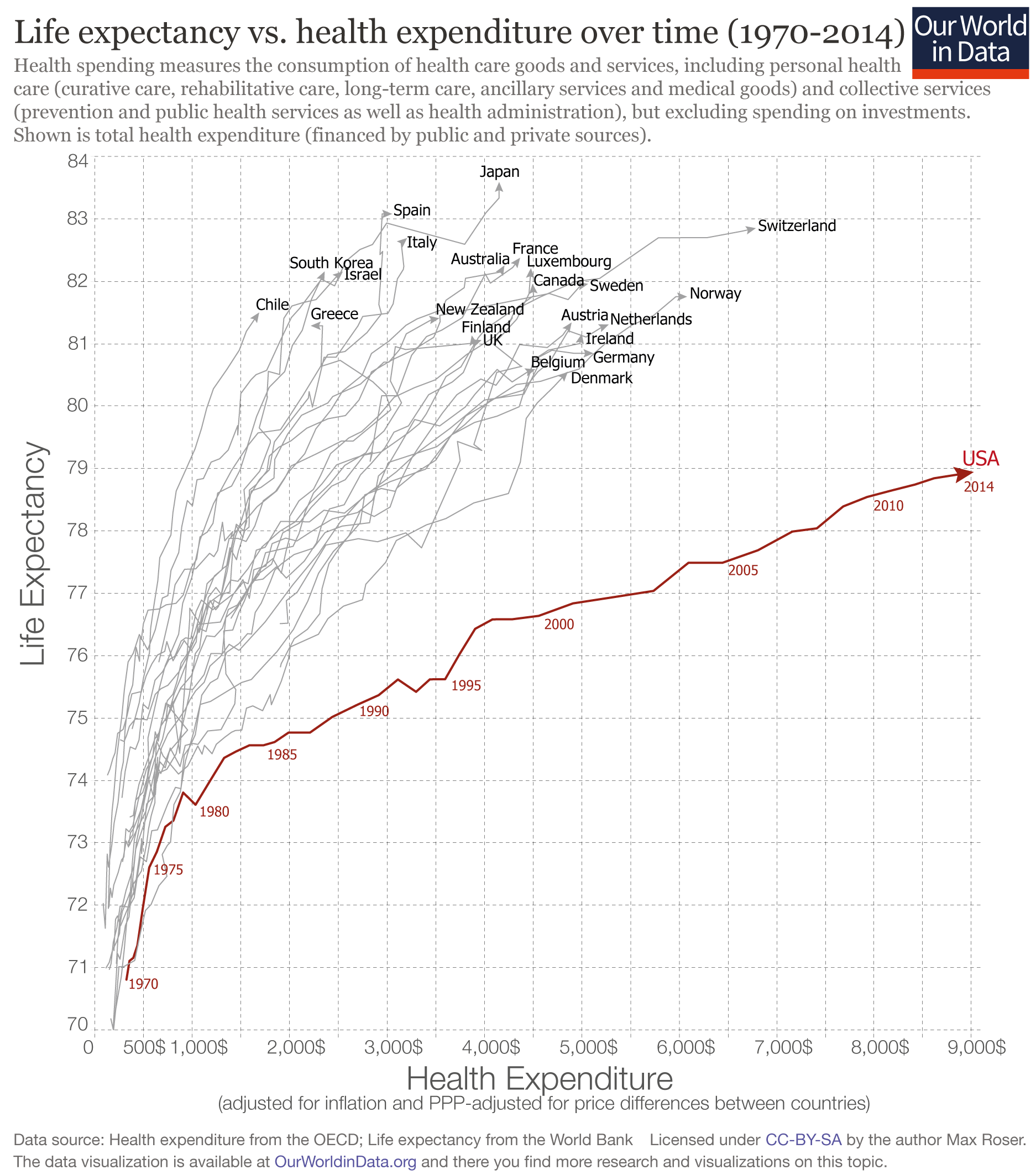
- QUOTE: The following graph visualizes the relationship between life expectancy and health expenditure, for a number of OECD countries across the period 1970-2014. Two points are worth mentioning. Firstly, all countries in this graph have followed an upward trajectory (life expectancy increased as health expenditure increased), but the U.S. stands out as an exception following a much flatter trajectory; gains in life expectancy from additional health spending in the U.S. were much smaller than in the other high-income countries, particularly since the mid-1980s. And secondly, the gains for all countries (except for the U.S.) were not diminishing, as in the previous graph. This suggests that there are many other factors affecting life expectancy, that are not determined by healthcare spending. Indeed, as we have pointed out before, healthcare is just one of many inputs to produce health.
- QUOTE: The following graph visualizes the relationship between life expectancy and health expenditure, for a number of OECD countries across the period 1970-2014. Two points are worth mentioning. Firstly, all countries in this graph have followed an upward trajectory (life expectancy increased as health expenditure increased), but the U.S. stands out as an exception following a much flatter trajectory; gains in life expectancy from additional health spending in the U.S. were much smaller than in the other high-income countries, particularly since the mid-1980s. And secondly, the gains for all countries (except for the U.S.) were not diminishing, as in the previous graph. This suggests that there are many other factors affecting life expectancy, that are not determined by healthcare spending. Indeed, as we have pointed out before, healthcare is just one of many inputs to produce health.